Vasculitis
This chapter reviews over the large, medium, and small vessel vasculitis you may encounter as a future physician. Being able to recognize them and know treatment is a crucial skill.
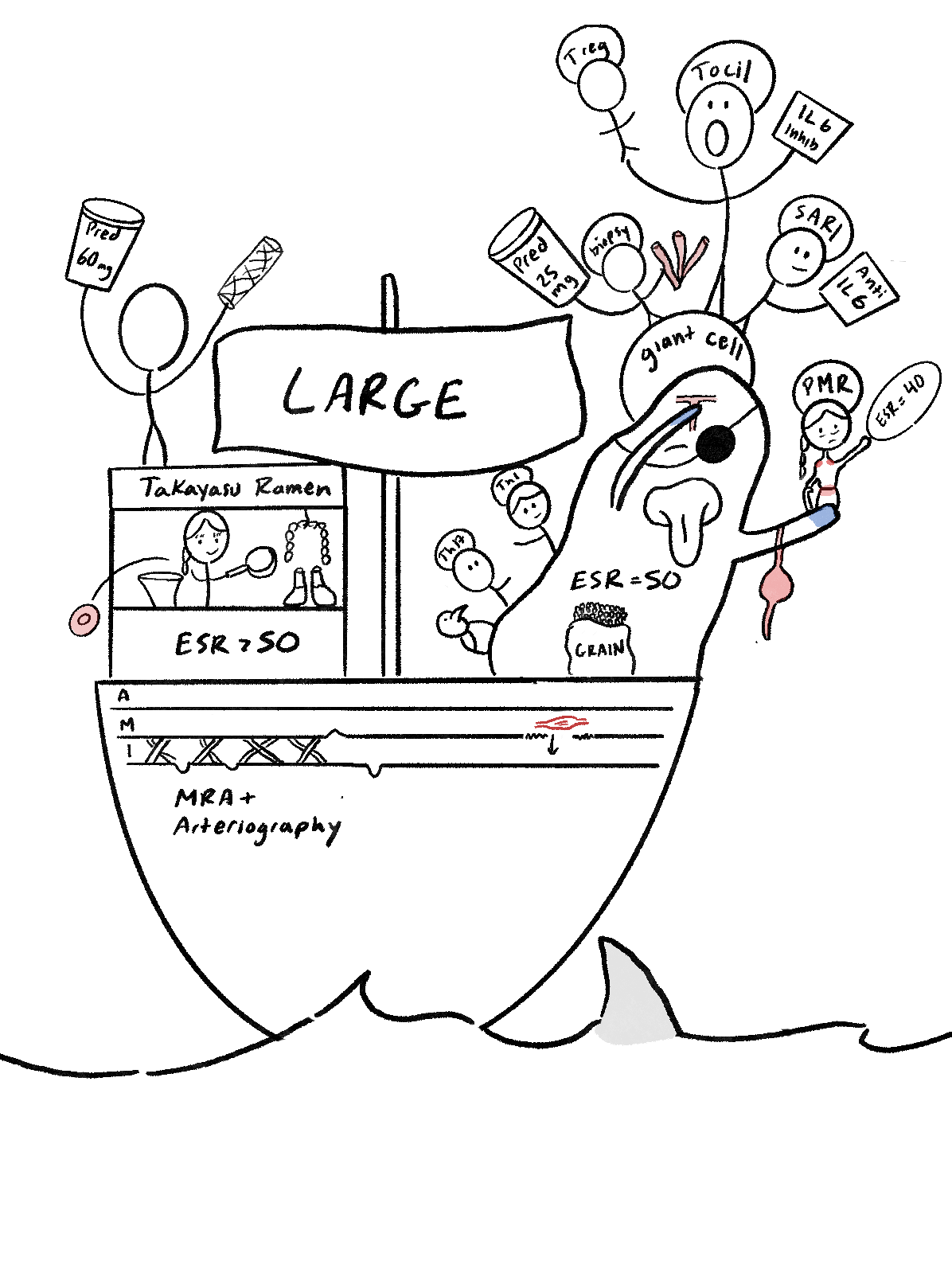
This is our large vessel vasculitis sketch. It features our giant cell and Takayasu ramen stand (Giant Cell arteritis and Takayasu arteritis). These are T lymphocyte responses and granuloma-forming vasculitis.
Let’s first look at our giant cell friend labeled “PMR” (polymyalgia rheumatica is an inflammatory condition). She is an older woman (usually affects older women). She has redness in her shoulder and hip (shoulder and hip girdle pain). This leads to myalgia and arthralgia (pain of muscles and joints). Note that PMR is NOT a vasculitis but accompanies Giant Cell often. She is holding a surfboard (ESR = 40 on lab values for PMR).
Let us move to our giant cell monster. He has his hand on head, eye patch, blue arms, tongue sticking out, and is over a “JAW-movie inspired” shark in the water (symptoms of giant cell include headache, blurred vision, cyanosis, and tongue or jaw claudication). On his head is a T-shaped blood vessel (Temporal artery is usually nodular, tender, and thick). On the monster’s belly is a tattoo (ESR = 50 for GCA). On his back are the immune cells involved (T-helper 1 and 17, as well as maCROWphages are involved in the pathogenesis). There is a sack of grains (Granulomas can be seen in GCA). Under the ship, a muscle cell goes into the intima (the internal elastic lamina is broken, allowing smooth muscle cells to invade).
Our biopsy guy on the monster head has three vessels (3 cm of the temporal artery is recommended for biopsy). The biopsy guy is holding PRED 25 (recommend treating with prednisone 12.5 to 25 mg a day tapered over a year). There are two more individuals (Sarilumab and Tocilizumab are both IL-6 monoclonal antibodies that are steroid sparing).
Now off to our last character, who is selling ramen. It is our Takayasu ramen. Notice it is a younger woman (affects women younger than 50). Takayasu is a Japanese ramen place (disease more common in Asia. However, it is not racially or geographically limited). Some meats are hanging in an ARCH over two lung-shaped jars (disease affects the aortic arch, pulmonary, and abdominal artery). There is a sign on the stand (ESR > 50 for this disease). Notice there is fibrosis going on in the intima of the ship vessel.
The girl also tosses a red blood cell into the ocean (disease causes anemia). A guy standing on top has a bottle of drugs and a stent (treatment for Takayasu includes prednisolone 60 mg a day. If it does not improve, may consider surgical intervention like angioplasty to open up stenosis). Finally, at the bottom of the ship, there are a few words “MRA + Arteriography” (MRA and arteriography are used for the diagnosis of the disease).

This is our medium-sized vessel vasculitis, including our PAN and TAO guy (polyarteritis nodosum and thromboangitis obliterans). First we will start with PAN. Notice that it is an older male (affects mostly older males). He is cooking some beans, stomach, and a nerve (PAN affects renal, abdominal, nerves, and skin). We did not draw in the skin, but just think about nerve endings on the skin. Notice there is a medium mast sign (it affects medium vessels). Our guy looks sweaty and throws a weight into the sea (symptoms include fever, malaise, and weight loss). His hand is all bent (mononeuritis multiplex). His other hand has dots (subcutaneous nodules). And his pants are purple (palpable purpura).
There is a sign next to our PAN guy (no lung involvement, no granulomas or eosinophilia in PAN). A tree next to the sign has a division with a dying flower (necrotizing inflammation involves bifurcations or branchings of arteries). On the side is our “B” hippo (hepatitis B is associated with this disease). Notice below deck, there are IgM binding to antigens (hepatitis IgM antibodies found in the blood walls). Notice there is release of complement as a result, including C5a (attracting neutrophils into the vessel wall to phagocyte the immune complex and leading to damaged walls). Notice that after the Neutrophils invade, our maCROWphage is next, leading to fibrosis, hence why we taped him to the wall of the ship.
The fibrosis or scarring of the blood vessel walls leads to narrowing, and aneurysmal dilation is commonly seen on angioGRAM. For diagnosis we have someone getting a biopsy from the hippo’s sural nerve and skin. For treatment, we have our “TREAT” guy. He is carrying a container of CS and CPP (treatment includes corticosteroids with cyclophosphamide). He also tosses a high-pressure tank into the ocean (should treat their hypertension as well). For labs, we take a look at the PAN guy tossing up CPR (C-reactive protein), WBC, and ESR > 50 (should see these labs elevated in PAN).
Moving on to our TAO guy. Our thromboangiitis obliterans has a burger (disease also called Buerger’s disease, but note this is different from the disease that causes IgA nephropathy). He is smoking (strong relationship with smoking). He is holding a sign (internal elastic lamina is preserved). Noice, TAO is in the small and medium-sized vessel (disease affects both small and medium). On the small vessel, we see that TAO has blue hands with black fingers (Raynaud’s phenomenon with gangrene is a common symptom). A PMN neutrophil guy jumps off and is replaced by a maCROWphage (pathogenesis includes PMNs being replaced with mononuclear cells like macrophages). The small vessel has a thrombus and fibrosis (TAO causes thrombus and fibrosis, leading to reduced pulses of the radial and ulnar). Hence why this is called an inflammatory OCCLUSIVE disorder. Recommend these patients to stop smoking.
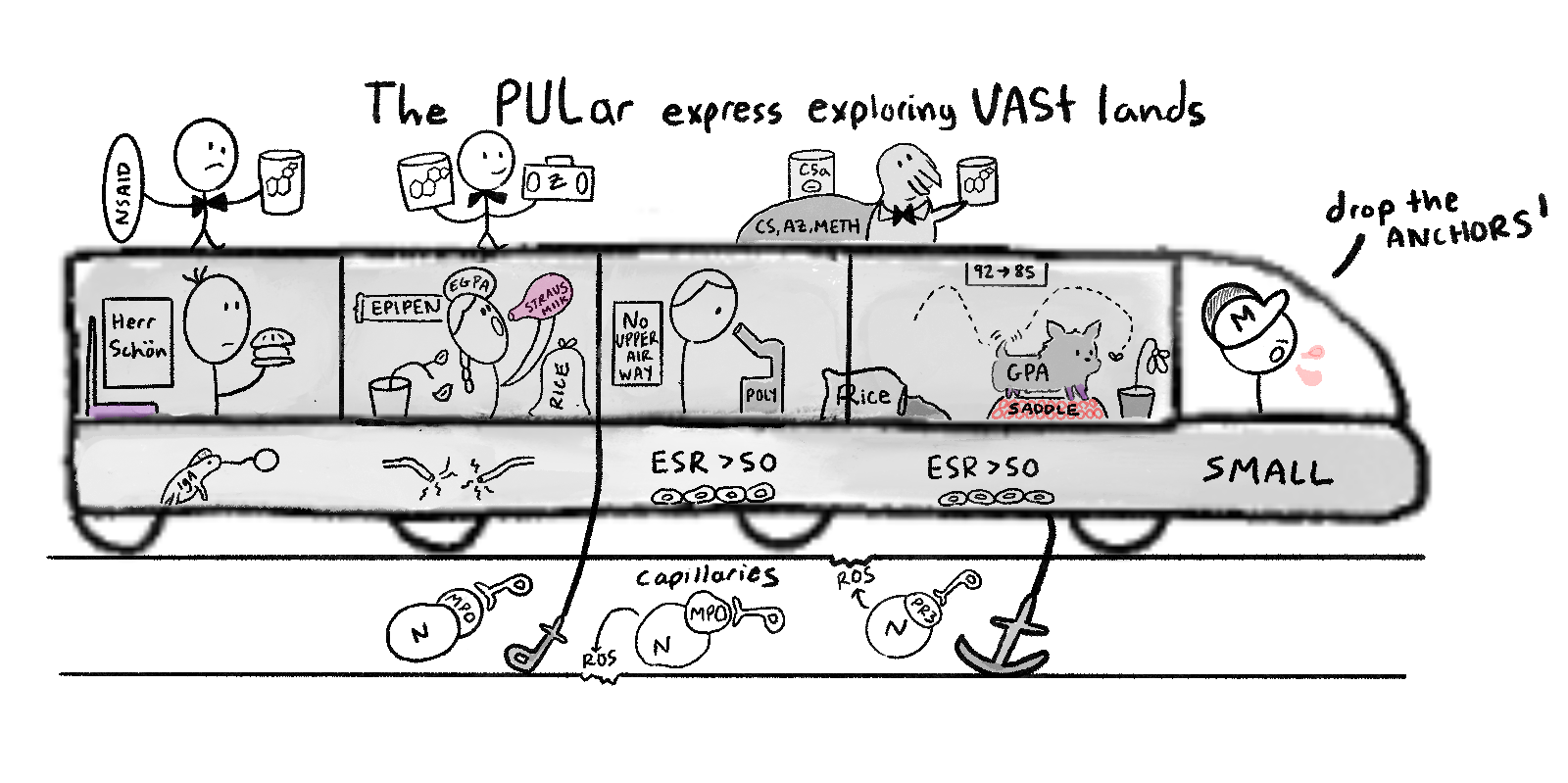
This is the PULAR EXPRESS, representing vasculitis for small vessels. This includes our four conditions, including Wegener’s (also called granulomatosis with polyangiitis), Microscopic Polyangiitis (MPA), Churg Strauss (Eosinophilic GPA), and Henoch Schonlein (IgA vasculitis). In summary, we added the treatments on top. Some important things to note is that our Wegener’s wagging dog is sitting on a saddle (saddle nose is classic finding). There is also a “NO upper airway” sign for MPA (does not affect the upper airway typically). And our Herr Schon guy has a purple seat (often seen palpable purpura of lower extremities). Also, our EGPA girl has a broken electric wire outside (mononeuritis multiplex is a common finding with inflamed nerve endings). Her milk is pink, as this is an eosinophilic reaction in the tissue and vessels. Also, notice that the MPO is the antigen for the two middle characters, while PR3 is the antigen for Wegener’s. Finally, for treatment, our walrus says CS, AZ, and METH (GPA and MPA treatments are the same, using high-dose corticosteroids with cyclophosphamide, then azathioprine, and methotrexate.) Our tuxes represent rituximab. And on the top of our dog is a sign that says 92 to 85 (95% have upper airway, while 85% have lower airway affected).
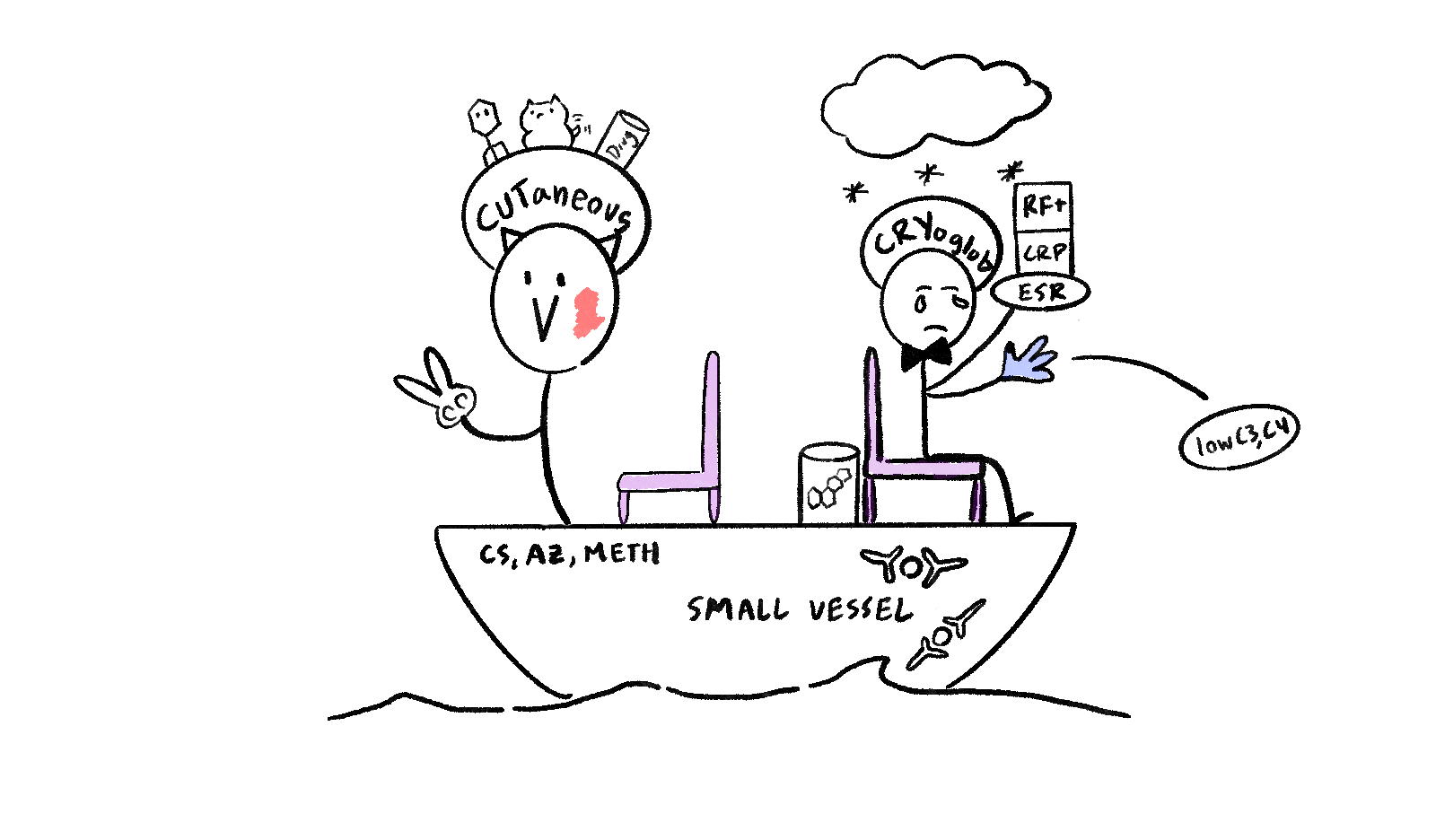
These are our two last small vessel vasculitis. On our right is our CRYglobulinemic vasculitis. There is snow and immune complexes forming on the ship wall (immune complexes form in the vessel wall in the cold). He is holding up ESR, CRP, and RF+ (elevated levels). Both conditions have a purple chair (palpable purpura). He has blue hands (Raynaud’s phenomenon, ulceration, and necrosis). He has steroids and a tux (treatment include corticosteroids and rituximab). He throws out complement (low complement levels).
Our other character is cutting stuff (cutaneous vasculitis). He is a wolf (seen in lupus). There is also a scar on his face (affects the dermis). And there is a virus, wagging dog, and drugs on his hat (these are associative causes of the disease). Finally treatment is CS, AZ, and METH (corticosteroids with taper, azathioprine, and methotrexate).