Cardiac Action Potentials
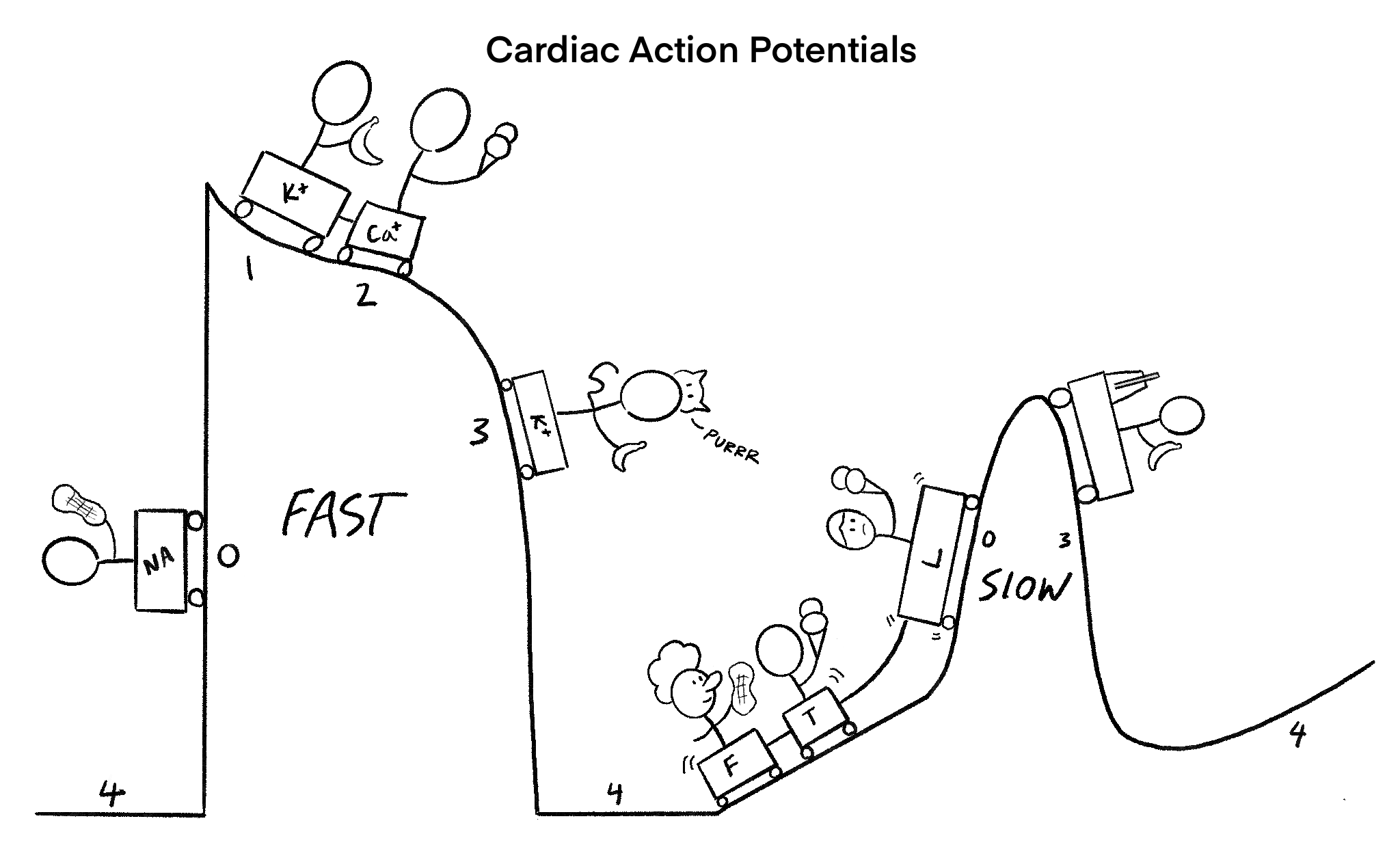
This is our cardiac action potential sketch, featuring our deadly rollercoaster. There are two types (fast and slow). It starts with our fast roller coaster on the LEFT. Notice our cart with the guy flexing with a cat (Fast action potentials are found in contractile cells and PURkinje cells). The fast rollercoaster starts with sodium rise, potassium fall, then a prolonged calcium influx, and finally a potassium efflux drop.
On the RIGHT is our slow rollercoaster. Notice the last guy with a metronome (slow action potential pattern found in pacemaker cells). It starts with our FUNNY clown, then two guys eating calcium-filled ice-cream labeled “T” and “L” (slow starts with Funny Channels, allowing sodium influx, then a transient calcium and long calcium channel for further depolarization). Finally, our guy with a banana slides down (potassium efflux leads to re-polarization and hyper-polarization.
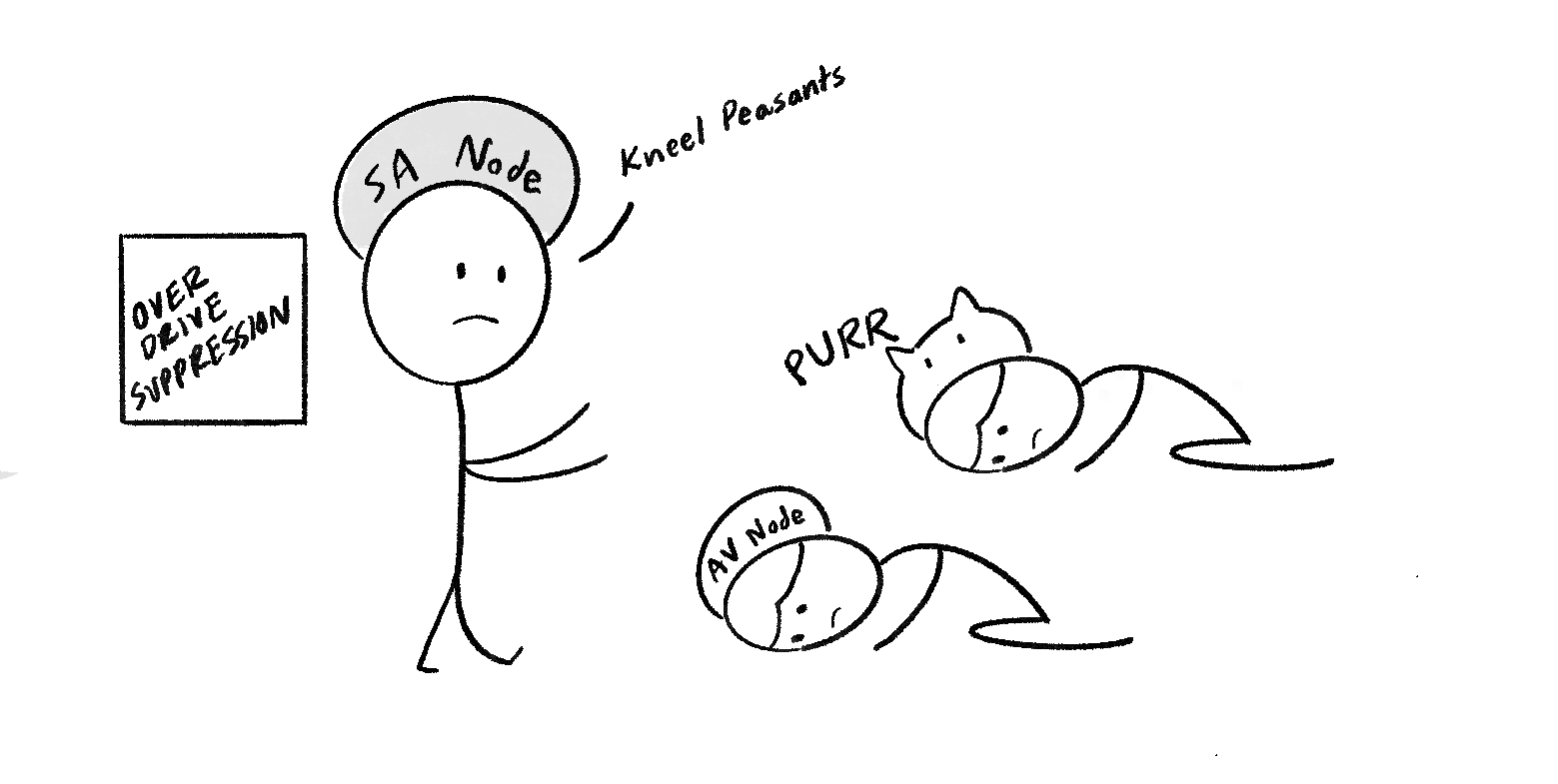
On the left is our depiction of overdrive suppression, where the SA node can suppress the activity of other pacemakers, allowing it to have a dominant effect on the heart rate.
On the side are our PURkinje cells and AV node getting suppressed by the AV node. Long live the AV node king.
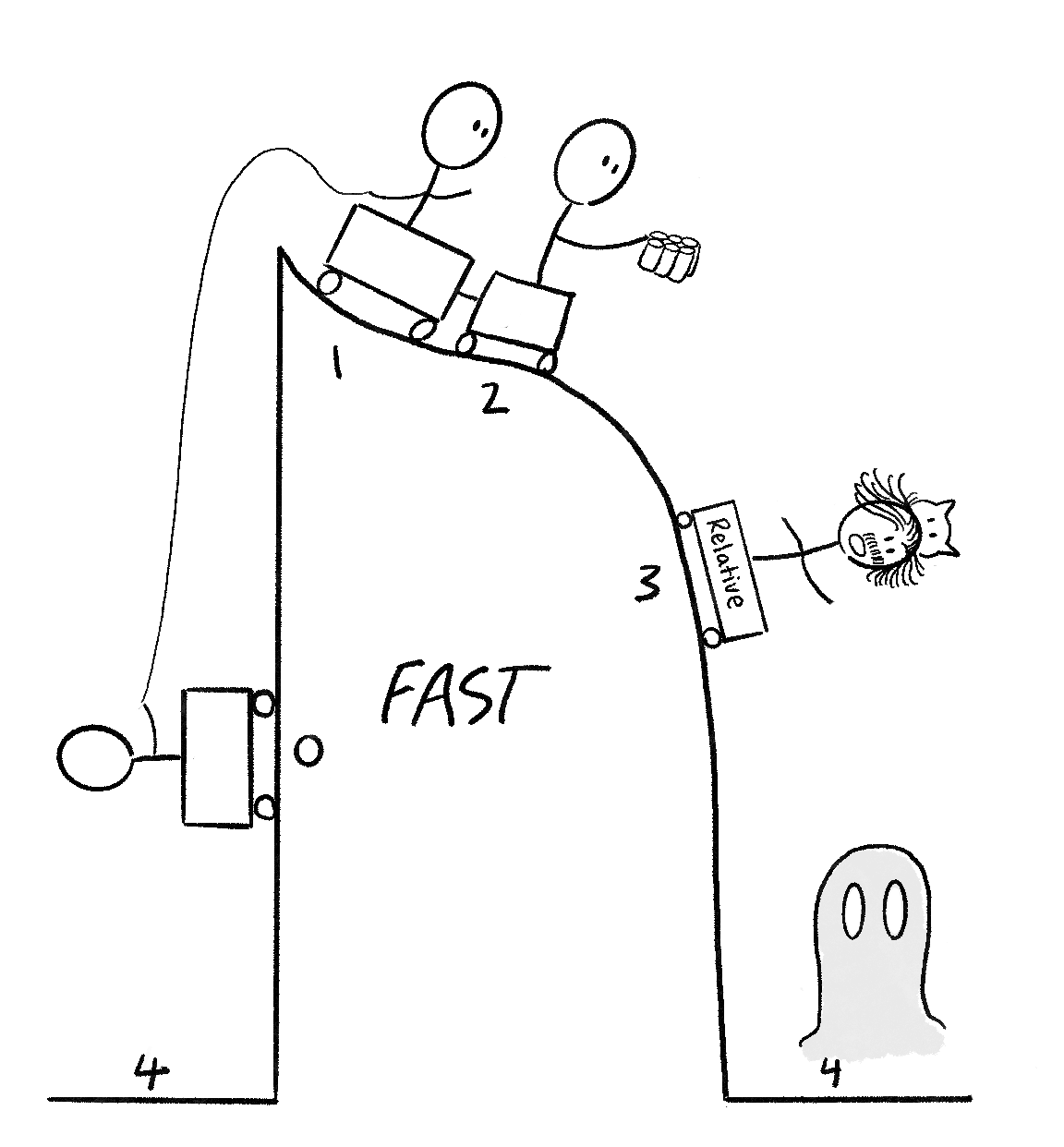
This sketch represents the difference between absolute, relative, and supernormal refractory periods. Notice our stages 0,1,2 are all connected with our lead person holding a 6-pack of drinks, similar to six pack ABS, or ABSOLUTE (0,1,2 is the absolute refractory period). Our stage three guy looks like Einstein, who discovered relativity (stage 3 is the effective/relative refractory period, where a stimulus may induce a small response. If it can propagate, it is considered the relative period). Finally, our paranormal ghost is chilling at stage 4 (a hyperexcitable period where a weaker-than-normal stimulus can cause an action potential).
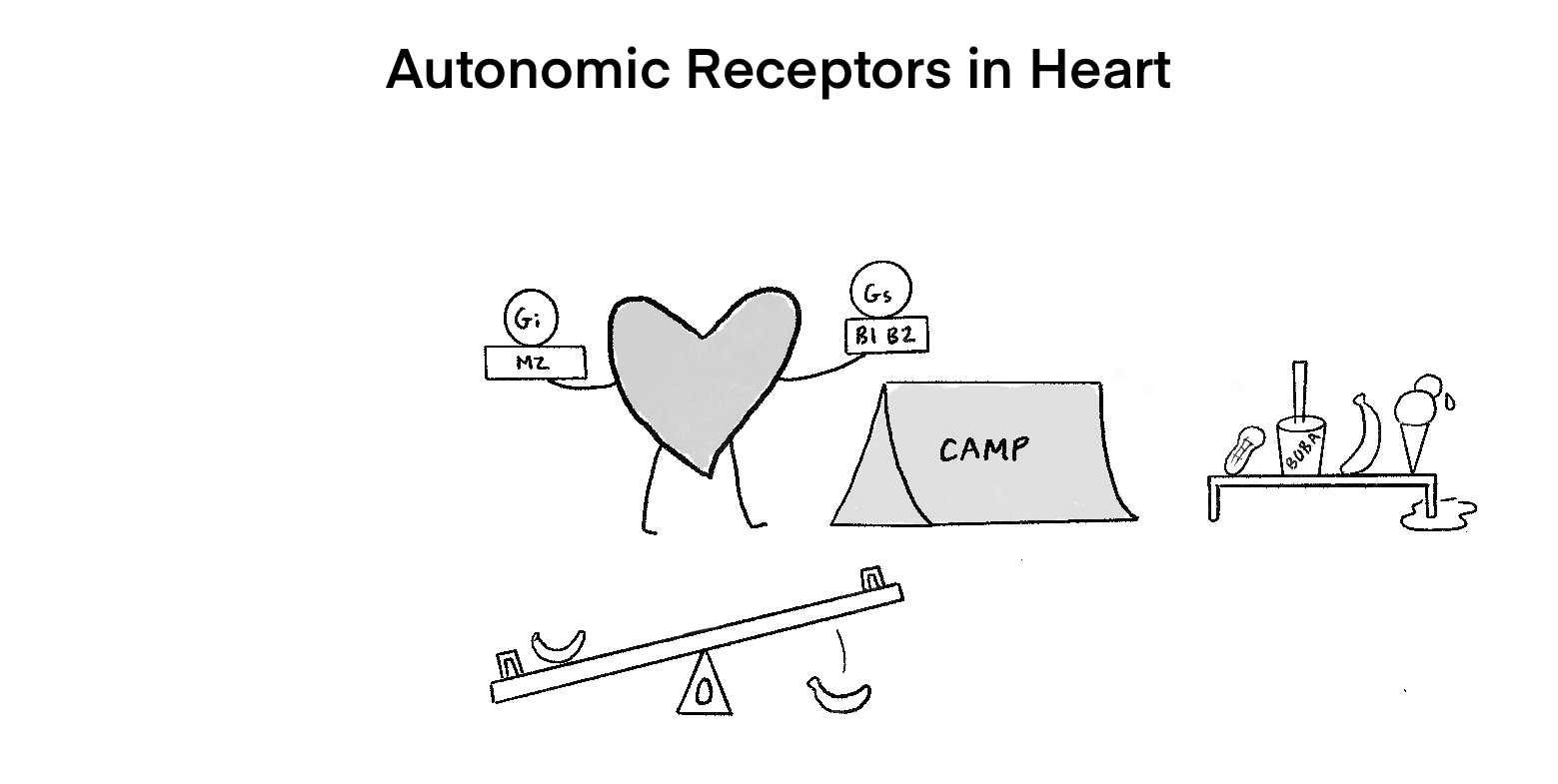
The heart has muscarinic cholinergic receptors and adrenergic receptors. Notice on the left is the M2 receptors, leading to Gi activation and less CAMP. On the other hand, our B1 and B2 receptors are activating Gs, increasing CAMP. Our seesaw represents the slope of the phase zero. In this case, the slope of 0 is increasing with sympathetic activation.
A banana is added on the left side, and a fallen one on the right (this represents how hyperkalemia causes a decrease in slope, while hypokalemia leads to an increase in slope 0. On the side are our antiarrhythmic drugs, including sodium-channel blockers, beta blockers, potassium channel blockers, and calcium channel blockers.
Think “Salty foam Boba with Banana Ice cream.”